Recent advances in physiotherapy for OA knee with current evidence based studies
OA (Osteo Arthritis) knee is a leading cause of pain and disability, which reduces the quality of life. The burden of the disease is expected to rise with an aged population and the increasing prevalence of obesity (Felson, 1). OA knee has been also a major cause of disability in older population.
Basically, OA knee is caused due to cartilage destruction. This cartilage loss is accompanied by bony remodeling which happens due to irregular body weight, capsular stretching which happens due to loading and unloading of joint and weakness of muscles in and around joints (Felson, 2). The cartilage destruction which occurs with OA is highly related due to disruption at cellular or molecular level rather than any other cause of external influence such as infection due to disease or recurrent trauma to joints due to falls or overuse of joints (Loeser, 3).
OA knee has 5 stages where the joint and the structure undergo changes. These stages are:
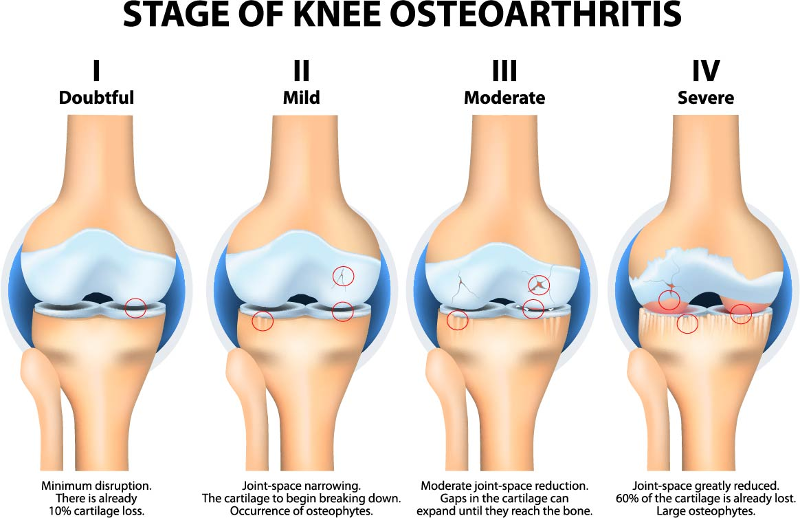
- Stage 0: Normal knee, no significant finding, normal healthy knee.
- Stage 1: A person with stage 1 OA is showing very minor bone spur growth. Bone spurs are boney growths that often develop where bones meet each other in the joint. Someone with stage1 OA will usually not experience any pain or discomfort as a result of the very minor wear on the components of the joint.
- Stage 2: Stage 2 OA of the knee is considered a “mild” stage of the condition X-rays of knee joints in this stage will reveal greater bone spur growth, but the cartilage is usually still at a healthy size, i.e. the space between the bones is normal, and the bones are not rubbing or scraping one another and patient has some discomfort only with few activities which requires exertion, e.g., running, jumping.
- Stage 3: Stage 3 OA is classified as “moderate” OA. In this stage, the cartilage between bones shows obvious damage, and the space between the bones begins to narrow. People with stage 3 OA of the knee are likely to experience frequent pain when walking, running, bending, or kneeling.
- Stage 4: Stage 4 OA is considered “severe.” People in stage 4 OA of the knee experience great pain and discomfort when they walk or move the joint. That’s because the joint space between bones is dramatically reduced, the cartilage is almost completely gone, leaving the joint stiff and possibly immobile. The synovial fluid is decreased dramatically, and it no longer helps reduce the friction among the moving parts of a joint.
The physiotherapist’s are among such professionals who can definitely help with initial stage of OA knee and can prevent the arthritic changes to occur for a longer duration.
Recent studies have shown the quality of knee could be improvised with physiotherapy provided the early diagnosis of OA knee. Studies have shown that with physiotherapy intervention and treatment such as modalities, which are machine-based physiotherapy, exercise therapy along with posture correction, proprioception and gait training the severity of OA progression and intensity of pain can be reduced among patients (4,5). Physiotherapy modalities such as Ultrasound (UST), IFT, SWD has definite effect on knee pain and discomfort when treating early stages of OA knee.The UST and IFT along with adjacent therapy such as exercise and posture correction are fruitful to get overall good outcome from the treatment. The UST has pulsed mode which is an intervention used to improve joint pain and improve joint movement quality in subjects with OA knee. The studies have shown the efficiency of treating OA knee is significant with initial mild to moderate stage of OA knee (6,7,8)
Exercise therapy includes the stretching, strengthening, and improve joint sense to maintain balance with activities. Stretching includes the stretch of muscle in and around knee joint. This improves flexibility of knee and activities such running, bending while stair climbing and squatting and others can be done efficiently. Strengthening includes of the muscle which are weak across the joint. This also includes the hip and ankle joint as well when treating the knee joint. The stretching and strengthening exercise would be different and unique based on the patient’s needs and will be designed accordingly by the physiotherapist based on his/her assessment (9,10).
The proprioception and gait training is an important parameter to treat in OA knee. The proprioception which is called joint sense, where the patient tends to understand the position of the joint movement is usually disturbed in OA knee patients. Gait which is the walking pattern is also disturbed in OA knee patient due to knee pain, obesity, malalignment (i.e., misalignment of bone segment on one over the other) of the bone are some reasons (11). Proper footwear correction through assessment can correct the malalignment of bone per studies which can also correct the knee and foot alignment and whereby prevent foot and knee pain problems (12).
Thus physiotherapy is definitely a treatment of choice in treating OA knee as a conservative mode of treatment. This also helps to prevent and delay severe arthritic changes and helps in betterment of knee if treated early. Hence, PT modalities and exercise are first treatment of choice among various conservative treatments per recent advances in healthcare. The overall physical and functional outcome is improved in patient with proper strengthening and muscle conditioning when followed physiotherapy protocol on regular basis.
References:
- Felson D.T., Anderson J.J., Naimark A., Walker A.M., Meenan R.F. (1988) Obesity and knee osteoarthritis. The Framingham Study. Ann Intern Med 109: 18–24 [PubMed]
- Felson D.T. (2009) Developments in the clinical understanding of osteoarthritis. Arthritis Res Ther 11: 203. [PMC free article] [PubMed]
- Loeser R.F. (2006) Molecular mechanisms of cartilage destruction: mechanics, inflammatory mediators, and ageing collide. Arthritis Rheum 54: 1357–1360 [PMC free article] [PubMed]
- Roddy E., Doherty M. (2006) Changing life-styles and osteoarthritis: what is the evidence? Best Pract Res Clin Rheumatol 20: 81–97 [PubMed]
- Scharf H.P., Mansmann U., Streitberger K., Witte S., Kramer J., Maier C., et al. (2006) Acupuncture and knee osteoarthritis: a three-armed randomized trial. Ann Intern Med 145: 12–20 [PubMed]
- Cakir S1, Hepguler S, Ozturk C, Korkmaz M, Isleten B, Atamaz FC. Efficacy of therapeutic ultrasound for the management of knee osteoarthritis: a randomized, controlled, and double-blind study.
- Zeng C1, Li H2, Yang T2, Deng ZH2, Yang Y2, Zhang Y2, Ding X2, Lei GH3. Effectiveness of continuous and pulsed ultrasound for the management of knee osteoarthritis: a systematic review and network meta-analysis.
- Draper DO1, Klyve D2, Ortiz R3, Best TM4. Effect of low-intensity long-duration ultrasound on the symptomatic relief of knee osteoarthritis: a randomized, placebo-controlled double-blind study.
- Aline Mizusaki Imoto, Maria Stella Peccin, and Virgínia Fernandes Moça Trevisani. Quadriceps strengthening exercises are effective in improving pain, function and quality of life in patients with osteoarthritis of the knee.
- Oliveira AM1, Peccin MS, Silva KN, Teixeira LE, Trevisani VF. Impact of exercise on the functional capacity and pain of patients with knee osteoarthritis: a randomized clinical trial.
- Lim BW1, Hinman RS, Wrigley TV, Bennell KL. Varus malalignment and its association with impairments and functional limitations in medial knee osteoarthritis.
- Jody Riskowski, Ph.D.,1,2 Alyssa B. Dufour, M.A.,1,3 and Marian T. Hannan, D.Sc, M.P.H.1,2. Arthritis, Foot Pain & Shoe Wear: Current Musculoskeletal Research on Feet.
Dr.Savitha
Consultant Physiotherapist
Spectrum Physio (Kaggadasapura)
Consultant Physiotherapist
Spectrum Physio (Kaggadasapura)